Surgery to the Intestines (Bowel)
Surgery to remove part of the intestine (also known as bowel resection) is sometimes required to manage benign diseases (for example traumatic injuries, bowel volvulus, ischaemia) and malignant tumours of the small or large intestines. The part of bowel removed depends on the location of the abnormality and the extent of disease involving other adjacent parts of the intestines. Once the affected part of bowel is removed, the options subsequently are to join the two remaining ends, known as an anastomosis (Figure A) or the ends are brought out to the surface of the skin as a stoma (Figure B).
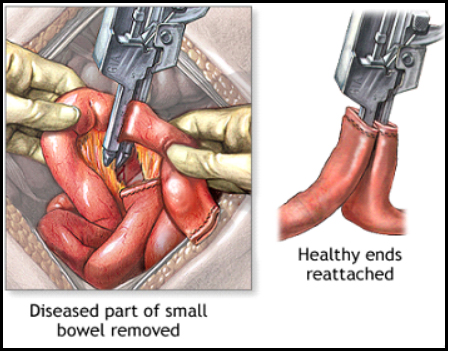
Figure A. Illustration of a bowel resection followed by formation of an anastomosis to restore bowel continuity.
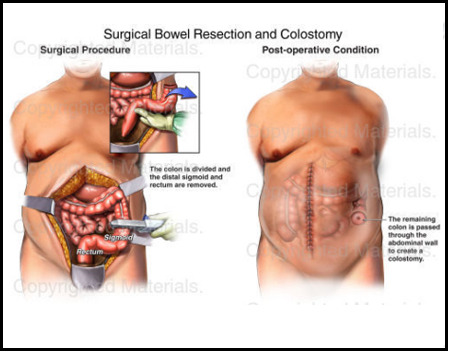
Figure B. Illustration of a bowel resection followed by formation of a stoma
Large Bowel Resections
In UMMC, we mainly perform surgery on the large bowel for the following conditions:
- Bowel cancer – this is the most common reason for the large bowel to be resected
- Diverticular disease – abnormal outpouching of the bowel wall
- Inflammatory bowel disease
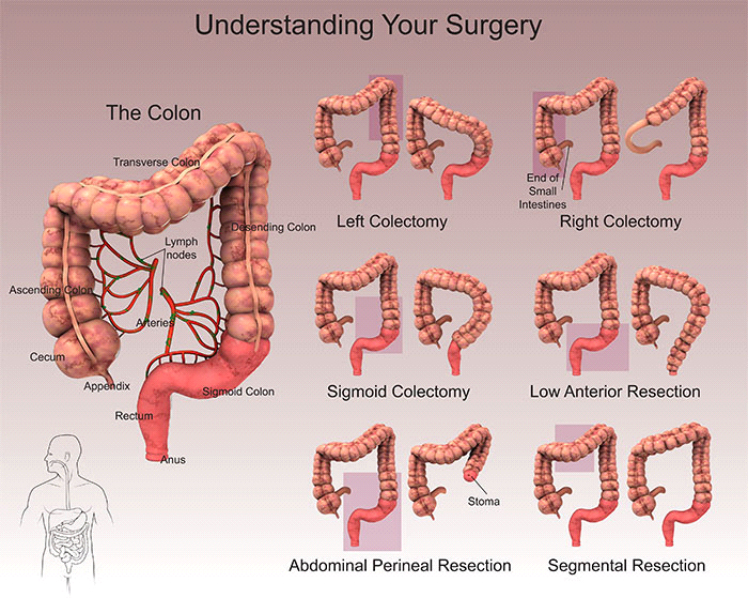
The type of surgery on the large bowel (colon) is commonly called a colectomy where part of the large bowel is resected. The segment of colon affected by disease will determine the type of operation performed as illustrated by the diagram below.
- Right hemicolectomy – part of or all of the ascending colon (right sided colon) and caecum are removed.
- Left hemicolectomy – part of or all of the descending colon (left sided colon) is removed.
- Sigmoid colectomy – part of or all of the sigmoid colon is removed.
- Anterior resection – the sigmoid colon and part of or all of rectum are removed. The colon is reconnected to remaining rectum or anus.
- Abdominoperineal resection – the sigmoid colon and part of or all of rectum are removed together with the anus. A stoma is created at the abdominal wall.

Assessment of the patient prior to elective colon resection includes evaluation of medical comorbidities, functional status, and social support. Planning intestine resection takes into account the nature of the lesion, its location within the intestine, and the status of the intestine circulation.
Preoperative assessment for patient with colorectal cancer may include a contrast-enhanced computed tomography (CT) scan of the thorax (lungs), abdomen and pelvis. For assessment of cancer involving rectum, MRI pelvis maybe necessary as well.
Potential complications of intestinal surgery might include surgical site infection, injury to surrounding structures (e.g. ureter, spleen), anastomotic leak, intra-abdominal abscess, enteric fistula, bleeding, and postoperative bowel obstruction, among others.